Ahonen, H., Deek, P., & Kroeker, J. (2012). Low frequency sound treatment promoting physical and emotional relaxation: A qualitative study. International Journal of Psychosocial Rehabilitation, 17(1), 45–58.
Ahonen-Eerikäinen, H. (1996). PAM – Psykoauditiivinen musiikkiterapiamenetelma. Musiikkiterapia, 1, 33-45.
Ala-Ruona, E. (2003). Fysioakustinen hoito osana erikoissairaanhoitoa ja kuntoutustutkimusta [The physioacoustic treatment as a part of specialized health care and rehabilitation assessment]. Muistoissa Petri Lehikoinen, 173-193.
Ala-Ruona, E., Punkanen, M., & Campbell, E. (2015). Vibroacoustic therapy: Conception, development, and future directions. Musiikkiterapia, 30(1-2), 48-71.
Ali, N., & Nater, U. M. (2020). Salivary alpha amylase as a biomarker of stress in behavioural medicine. International Journal of Behavioral Medicine, 27(3), 337–342. https://doi.org/10.1007/s12529-019-09843-x
Almeida, Q., King, L., & Ahonen-Eerikainen, H. (2007). Short-term Influences of the Physioacoustic Method on Symptoms in Parkinson's Disease. Neurorehabilitation and Neural Repair.
Almeida-Santos, M. A., Barreto-Filho, J. A., Oliveira, J. L. M., Reis, F. P., da Cunha Oliveira, C. C., & Sousa, A. C. S. (2016). Aging, heart rate variability and patterns of autonomic regulation of the heart. Archives of gerontology and geriatrics, 63, 1-8.
Annunziata, M. L., Scala, M., Giuliano, N., Tagliaferri, S., Imperato, O. C. M., Esposito, F. G., Campanile, M., & Di Lieto, A. (2012). Fetal Vibroacoustic Stimulation in Computerized Cardiotocographic Analysis: The Role of Short-Term Variability and Approximate Entropy. Journal of Pregnancy, 2012, 814987. https://doi.org/10.1155/2012/814987
Bailey, B., Gravel, J., & Daoust, R. (2012). Reliability of the visual analog scale in children with acute pain in the emergency department. PAIN®, 153(4), 839-842.
Bartel, L. R., Chen, R., Alain, C., & Ross, B. (2017). Vibroacoustic stimulation and brain oscillation: From basic research to clinical application. Music and Medicine, 9(3), 153-166.
Bartel, L., & Mosabbir, A. (2021). Possible mechanisms for the effects of sound vibration on human health. In Healthcare (Vol. 9, No. 5, p. 597). MDPI.
Benson, H. (1975). The Relaxation Response. William Morrow and Company.
Bergström-Isacsson, M., Lagerkvist, B., Holck, U., & Gold, C. (2014). Neurophysiological responses to music and vibroacoustic stimuli in Rett syndrome. Research in developmental disabilities, 35(6), 1281-1291.
Bilan, A., Witczak, A., Palusiński, R., Myśliński, W., & Hanzlik, J. (2005). Circadian rhythm of spectral indices of heart rate variability in healthy subjects. Journal of electrocardiology, 38(3), 239-243.
Blomqvist, M., Holmberg, K., Lindblad, F., Fernell, E., Ek, U., & Dahllöf, G. (2007). Salivary cortisol levels and dental anxiety in children with attention deficit hyperactivity disorder. European Journal of Oral Sciences, 115(1), 1-6.
Boucsein, W. (2012). Electrodermal activity. Springer Science & Business Media.
Boyd-Brewer, C., & McCaffrey, R. (2004). Vibroacoustic sound therapy improves pain management and more. Holistic Nursing Practice, 18(3), 111–118. https://doi.org/10.1097/00004650-200405000-00009
Brabant, O., van de Ree, M., & Erkkilä, J. (2017). The effect of resonance frequency breathing when used as a preparatory exercise in music psychotherapy: A single-case experimental study of a client with anxiety disorder. The Arts in Psychotherapy, 56, 7–18. https://doi.org/10.1016/j.aip.2017.08.004
Brabcová, D. B., & Kohout, J. (2018). PSYCHOMETRICKÉ OVĚŘENÍ ČESKÉ VERZE ŠKÁLY VNÍMANÉHO STRESU. E-psychologie, 12(1).
Braunlin, E. A., Harmatz, P. R., Scarpa, M., Furlanetto, B., Kampmann, C., Loehr, J. P., Ponder, K. P., Roberts, W. C., Rosenfeld, H. M., & Giugliani, R. (2011). Cardiac disease in patients with mucopolysaccharidosis: presentation, diagnosis and management. Journal of inherited metabolic disease, 34(6), 1183–1197.
Bressler, S. L. (1990). The gamma wave: A cortical information carrier? Trends in Neurosciences, 13(5)[143], 161–162. https://doi.org/10.1016/0166-2236(90)90039-D
Brown, C. J., Chen, A. C., & Dworkin, S. F. (1989). Music in the control of human pain. Music therapy, 8(1), 47-60.
Buchheit M. (2014). Monitoring training status with HR measures: do all roads lead to Rome?. Frontiers in physiology, 5, 73.
Campbell, E. A. (2019). Vibroacoustic treatment and self-care for managing the chronic pain experience: an operational model. JYU dissertations.
Campbell, E. A., Hynynen, J., & Ala-Ruona, E. (2017). Vibroacoustic treatment for chronic pain and mood disorders in a specialized healthcare setting. Music and Medicine, 9(3), 187-197.
Campbell, E. A., Hynynen, J., Burger, B., & Ala-Ruona, E. (2019). Exploring the use of Vibroacoustic treatment for managing chronic pain and comorbid mood disorders: A mixed methods study. Nordic Journal of Music Therapy, 28(4), 291-314.
Campbell, E., Hynynen, J., Burger, B., Vainionpää, A., and Ala-Ruona, E. (2019). Vibroacoustic treatment to improve functioning and ability to work: A multidisciplinary approach to chronic pain rehabilitation. Disabil. Rehabil. 43, 2055–2070. doi: 10.1080/09638288.2019.1687763
Campbell, E., Burger, B., & Ala-Ruona, E. (2019). A single-case, mixed methods study exploring the role of music listening in vibroacoustic treatment. In Voices: A World Forum for Music Therapy (Vol. 19, No. 2, pp. 27-27).
Cannon, W. B. (1932). The Wisdom of the Body. New York: W.W. Norton.
Carrington, M. J., Barbieri, R., Colrain, I. M., Crowley, K. E., Kim, Y., & Trinder, J. (2005).
Changes in cardiovascular function during the sleep onset period in young adults. Journal of Applied Physiology, 98(2), 468-476.
Cohen, J. (1988). Statistical power analysis for the behavioral sciences (2nd ed.). Lawrence Erlbaum Associates.
Cohen, S., Janicki-Deverts, D., & Miller, G. E. (2007). Psychological stress and disease. JAMA, 298(14), 1685–1687. https://doi.org/10.1001/jama.298.14.1685
Cohen, S., Kamarck, T., & Mermelstein, R. (1983). A global measure of perceived stress. Journal of Health and Social Behavior, 24(4), 385–396. https://doi.org/10.2307/2136404
Corbett, B. A., Mendoza, S., Abdullah, M., Wegelin, J. A., & Levine, S. (2006). Cortisol circadian rhythms and response to stress in children with autism. Psychoneuroendocrinology, 31(1), 59–68. https://doi.org/10.1016/j.psyneuen.2005.05.011
Couper, M. P., Tourangeau, R., Conrad, F. G., & Singer, E. (2006). Evaluating the effectiveness of visual analog scales: A web experiment. Social Science Computer Review, 24(2), 227-245.
Craig, A. D. (2002). How do you feel? Interoception: The sense of the physiological condition of the body. Nature Reviews Neuroscience, 3(8), 655–666. https://doi.org/10.1038/nrn894
Critchley, H. D. (2002). Electrodermal responses: What happens in the brain. The Neuroscientist, 8(2), 132–142. https://doi.org/10.1177/107385840200800209
Čadilová, V., & Žampachová, Z. (2012). Metodika práce se žákem s poruchami autistického spektra. Olomouc: Univerzita Palackého v Olomouci.
Delmastro, F., Di Martino, F., and Dolciotti, C. (2018). “Physiological impact of vibro-acoustic therapy on stress and emotions through wearable sensors,” in Proceedings of the 2018 IEEE international conference on pervasive computing and communications workshops (IEEE) (Athens: IEEE), 621–626.
DeLongis, A., Coyne, J. C., Dakof, G., Folkman, S., & Lazarus, R. S. (1982). Relationship of daily hassles, uplifts, and major life events to health status. Health Psychology, 1(2), 119–136. https://doi.org/10.1037/0278-6133.1.2.119
Dickerson, S. S., & Kemeny, M. E. (2004). Acute stressors and cortisol responses: A theoretical integration and synthesis of laboratory research. Psychological Bulletin, 130(3), 355–391. https://doi.org/10.1037/0033-2909.130.3.355
Duck, F. A. (1990). Physical properties of tissues: A comprehensive reference book. Academic Press.
Dudonienė, V., Budrienė, L., Aukštikalnis, T., Lendraitienė, E., Čerkauskas, J., & Raistenskis, J. (2016). Effect of vibroacoustic therapy on pain management in adolescents with low back pain.
Faul, F., Erdfelder, E., Lang, A. G., & Buchner, A. (2007). G*Power 3: a flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behavior Research Methods, 39, 175-191.
Fooks, C., & Niebuhr, O. (2024). Effects of Vibroacoustic Stimulation on Psychological, Physiological, and Cognitive Stress. Sensors, 24(18), 5924.
Friedlová, K. (2007). Bazální stimulace v základní ošetřovatelské péči. Grada Publishing as.
Fritz, C. O., Morris, P. E., & Richler, J. J. (2012). Effect size estimates: current use, calculations, and interpretation. Journal of experimental psychology: General, 141(1), 2.
Galambos, R., Makeig, S., & Talmachoff, P. J. (1981). A 40-Hz auditory potential recorded from the human scalp. Proceedings of the national academy of sciences, 78(4), 2643-2647.
Gąsior, J. S., Zamunér, A. R., Silva, L. E. V., Williams, C. A., Baranowski, R., Sacha, J., Machura, P., Kochman, W., & Werner, B. (2020). Heart Rate Variability in Children and Adolescents with Cerebral Palsy-A Systematic Literature Review. Journal of clinical medicine, 9(4), 1141.
Gendlin, E. T. (1969). Focusing. Psychotherapy: Theory, Research & Practice, 6(1), 4.
Ghasemi, A., & Zahediasl, S. (2012). Normality tests for statistical analysis: a guide for non-statisticians. International journal of endocrinology and metabolism, 10(2), 486–489.
Goetz, M., & Uhlíková, P. (2009). ADHD-porucha pozornosti s hyperaktivitou: příručka pro starostlivé rodiče a zodpovědné učitele. Galén.
Grassmann, M., Vlemincx, E., von Leupoldt, A., Mittelstädt, J. M., & Van den Bergh, O. (2016). Respiratory changes in response to cognitive load: a systematic review. Neural Plasticity, 2016, Article 8146809. https://doi.org/10.1155/2016/8146809
Grocke, D., & Wigram, T. (2006). Receptive methods in music therapy: Techniques and clinical applications for music therapy clinicians, educators and students. Jessica Kingsley Publishers.
Haltia, M. (2003). The neuronal ceroid-lipofuscinoses. Journal of Neuropathology & Experimental Neurology, 62(1), 1–13. https://doi.org/10.1093/jnen/62.1.1ScienceDirect+2
Hartley, S. L., & MacLean, W. E. (2005). Perceptions of stress and coping strategies among adults with mild mental retardation: Insight into psychological distress. American Journal on Mental Retardation, 110(4), 285–297. https://doi.org/10.1352/0895-8017(2005)110[285:POSACS]2.0.CO;2
Hayes, M. H. S., & Patterson, D. G. (1921). Experimental development of the graphic rating method. Psychological Bulletin, 18(1), 98–99
Hellhammer, D. H., Wüst, S., & Kudielka, B. M. (2009). Salivary cortisol as a biomarker in stress research. Psychoneuroendocrinology, 34(2), 163–171. https://doi.org/10.1016/j.psyneuen.2008.10.026
Holmes, T. H., & Rahe, R. H. (1967). The Social Readjustment Rating Scale. Journal of Psychosomatic Research, 11(2), 213–218. https://doi.org/10.1016/0022-3999(67)90010-4
Hooper, J. (2001). Is vibroacoustic therapy music therapy? Music Therapy Perspectives, 19(1), 68–74.
Hooper, J., Wigram, T., Carson, D., & Lindsay, B. (2008). A review of the music and intellectual disability literature (1943–2006) part two—experimental writing. Music Therapy Perspectives, 26(2), 80-96.
Howard, D., & Angus, J. (2009). Acoustics and psychoacoustics. Routledge.
Hrdlička, M., & Komárek, V. (2004). Dětský autismus: přehled současných poznatků. Praha: Portál.
Chesky, K. S., & Michel, D. E. (1996). The music vibration table: a possible innovative form of pain relief, especially for the performing artist. Medical Problems of Performing Artists, 11(1), 30-34.
Chesky, K., Rubin, B., & Frische, E. (1992). The Pain Relieving Effect of Music Vibration on Rheumatoid Arthitis Patients as Related to Just Music and Placebo. ISME conference, book of abstracts.
Chrousos, G. P. (2009). Stress and disorders of the stress system. Nature Reviews Endocrinology, 5(7), 374–381. https://doi.org/10.1038/nrendo.2009.106
Iob, E., & Steptoe, A. (2019). Cardiovascular disease and hair cortisol: a novel biomarker of chronic stress. Current Cardiology Reports, 21(10), 116. https://doi.org/10.1007/s11886-019-1208-7
Kanner, A. D., Coyne, J. C., Schaefer, C., & Lazarus, R. S. (1981). Comparison of two modes of stress measurement: Daily hassles and uplifts versus major life events. Journal of Behavioral Medicine, 4(1), 1–39. https://doi.org/10.1007/BF00844845
Kantor, J., Hlaváčková, L., Du, J., Dvořáková, P., Svobodova, Z., Karasová, K., & Kantorova, L. (2022). The effects of Ayres sensory integration and related sensory based interventions in children with cerebral palsy: a scoping review. Children, 9(4), 483.
Kantor, J., Campbell, E. A., Kantorová, L., Marečková, J., Regec, V., Karasová, K., ... & Klugar, M. (2022). Exploring vibroacoustic therapy in adults experiencing pain: a scoping review. BMJ open, 12(4), e046591.
Kantor, J. (2014). Kreativní přístupy v rehabilitaci osob s těžkým kombinovaným postižením: výzkumy, teorie a jejich využití v edukaci a terapiích. Univerzita Palackého v Olomouci.
Katmah, R., Al-Shargie, F., Tariq, U., Babiloni, F., Al-Mughairbi, F., & Al-Nashash, H. (2021). A review on mental stress assessment methods using EEG signals. Sensors, 21(15), 5043. https://doi.org/10.3390/s21155043
Katusic, A., Alimovic, S., & Duranovic, V. (2013). The effect of vibration therapy on spasticity and motor function in children with cerebral palsy: A randomized controlled trial. Neurorehabilitation, 32(1), 163-172. https://doi.org/10.3233/NRE-130817
Katušić, A., & Mejaški-Bošnjak, V. (2011). Effects of vibrotactile stimulation on the control of muscle tone and movement facilitation in children with cerebral injury. Collegium antropologicum, 35(1), 57-63.
Kędzierska, K., Synder, M., & Kozłowski, P. (2021). Influence of Vibroacoustic Therapy on Local Status and Rehabilitation of Post-TKR and Post-THR Patients. Ortopedia, Traumatologia, Rehabilitacja, 23(2), 101–113. https://doi.org/10.5604/01.3001.0014.8139
Khalfa, S., Peretz, I., Blondin, J.-P., & Manon, R. (2002). Event-related skin conductance responses to musical emotions in humans. Neuroscience Letters, 328(2), 145–149. https://doi.org/10.1016/S0304-3940(02)00462-7
Kim, H. G., Cheon, E. J., Bai, D. S., Lee, Y. H., & Koo, B. H. (2018). Stress and heart rate variability: A meta-analysis and review of the literature. Psychiatry Investigation, 15(3), 235–245. https://doi.org/10.30773/pi.2017.08.17
Kim, S. A., & LCAT, M. B. (2013). Stress reduction and wellness.
Kinsler, L. E., Frey, A. R., Coppens, A. B., & Sanders, J. V. (2000). Fundamentals of acoustics. John wiley & sons.
Kirschbaum, C., & Hellhammer, D. H. (1994). Salivary cortisol in psychoneuroendocrine research: Recent developments and applications. Psychoneuroendocrinology, 19(4), 313–333. https://doi.org/10.1016/0306-4530(94)90013-2
Koenig, J., & Thayer, J. F. (2016). Sex differences in healthy human heart rate variability: A meta-analysis. Neuroscience & Biobehavioral Reviews, 64, 288–310. https://doi.org/10.1016/j.neubiorev.2016.03.007
Koike, Y., Hoshitani, M., Tabata, Y., Seki, K., Nishimura, R., & Kano, Y. (2012). Effects of vibroacoustic therapy on elderly nursing home residents with depression. Journal of Physical therapy science, 24(3), 291-294.
Kraus, J. (2005). Dětská mozková obrna. Grada Publishing, as.
Kyriacou, C. (2001). Teacher stress: Directions for future research. Educational Review, 53(1), 27-35.
Lazarus, R. S., & Folkman, S. (1984). Stress, appraisal, and coping. New York: Springer Publishing Company.
Lehikoinen, P. (1998). The Physioacoustic Method. Acoustic Vibration in Medicine. Finnish Journal of Music Education, 3(3), 25-50.
Levenstein, S., Prantera, C., Varvo, V., Scribano, M. L., Berto, E., Luzi, C., & Andreoli, A. (1993). Development of the Perceived Stress Questionnaire: A new tool for psychosomatic research. Journal of Psychosomatic Research, 37(1), 19–32. https://doi.org/10.1016/0022-3999(93)90120-5
Liengme, B. & Hekman, K. (2020). Chapter 16 - Statistics for Experimenters. Liengme, B. & Hekman, K. (eds) Liengme's Guide to Excel® 2016 for Scientists and Engineers, Academic Press, pp. 371-396.
Llinas, R., & Ribary, U. (1993). Coherent 40-Hz oscillation characterizes dream state in humans. Proceedings of the National Academy of Sciences, 90(5), 2078-2081.
Lovallo, W. R. (2015). Stress and health: Biological and psychological interactions. Sage publications.
Lovibond, P. F., & Lovibond, S. H. (1995). Depression anxiety and stress scales. Behaviour Research and Therapy.
Łukasiak A, Krystosiak M, Widłak P, Woldańska-Okońska M. (2013) Ocena skuteczności leczenia pacjentów z tzw. ostrogą piętową z zastosowaniem terapii wibroakustycznej. Ortop Traumatol Rehabil;15(1):77-87.
Lundqvist, L.-O., Andersson, G., & Viding, J. (2009). Effects of vibroacoustic music on challenging behaviors in individuals with autism and developmental disabilities. Research in Autism Spectrum Disorders, 3(2), 390-400. https://doi.org/10.1016/j.rasd.2008.08.005
Macartney, M. J., McLennan, P. L., & Peoples, G. E. (2021). Heart rate variability during cardiovascular reflex testing: the importance of underlying heart rate. Journal of Basic and Clinical Physiology and Pharmacology, 32(3), 145-153.
Maihoefner, C., Reulbach, U., Doerfler, A., Fasching, P., Renner, S., Münster, T., ... & Sperling, W. (2010). Infarction of primary sensorimotor cortex impairs pain perception. Cerebrovascular Diseases (Basel, Switzerland), 30(2), 200-201.
Marshall, F. J., De Blieck, E. A., Mink, J. W., Kwon, J. M., & Augustine, E. F. (2005). Electrocardiographic and heart rate variability findings in juvenile neuronal ceroid lipofuscinosis. Pediatric Neurology, 33(3), 204–208. https://doi.org/10.1016/j.pediatrneurol.2005.03.015
McEwen, B. S. (2012). The brain on stress: How the social environment gets under the skin. Proceedings of the National Academy of Sciences, 109(Suppl. 2), 17180–17185. https://doi.org/10.1073/pnas.1121254109
McEwen, B. S. (2013). Allostasis and allostatic load: implications for neuropsychopharmacology. Stress and the Brain, 2-18.
McEwen, B. S., & Stellar, E. (1993). Stress and the individual: Mechanisms leading to disease. Archives of Internal Medicine, 153(18), 2093–2101.
Mole, S. E., & Cotman, S. L. (2015). Genetics of the neuronal ceroid lipofuscinoses (Batten disease). Biochimica et Biophysica Acta (BBA) - Molecular Basis of Disease, 1852(10 Pt B), 2237–2241. https://doi.org/10.1016/j.bbadis.2015.05.011
Moore, J., Farquharson, K., & Lotter, C. (2025, February). “Grooving in My Body”: A Mixed-Methods Pilot Study of Vibroacoustic Therapy’s Effects on Emotion Regulation and Attention in Autistic Children. In Healthcare (Vol. 13, No. 5, p. 465). MDPI.
Michalík, J., Baslerová, P., Felcmanová, L., & kol. (2015). Katalog podpůrných opatření: Dílčí část pro žáky s potřebou podpory ve vzdělávání z důvodu zdravotního nebo sociálního znevýhodnění. Univerzita Palackého v Olomouci. ISBN 978-80-244-4654-7.
Mind Garden. (n.d.). Perceived Stress Scale. Retrieved from https://www.mindgarden.com/documents/PerceivedStressScale.pdf
Nagai, N., Matsumoto, T., Kita, H., & Moritani, T. (2003). Autonomic nervous system activity and the state and development of obesity in Japanese school children. Obesity research, 11(1), 25-32.
Nepal, G. B., & Paudel, B. H. (2012). Effect of posture on heart rate variability in school children. Nepal Medical College journal : NMCJ, 14(4), 298–302.
Neuhaus, E., Bernier, R. A., & Beauchaine, T. P. (2016). Children with Autism Show Altered Autonomic Adaptation to Novel and Familiar Social Partners. Autism research : official journal of the International Society for Autism Research, 9(5), 579–591.
Neukirchen, T., Stork, M., Hoppe, M. W., & Vorstius, C. (2022). Spirometry has added value over electrodermal activity as a physiological marker of mental load in male subjects. Scientific Reports, 12(1), 4496. https://doi.org/10.1038/s41598-022-08480-x
Nosková, P. (2010). Chronická bolest, diagnostika, terapie. Interní medicína pro praxi, 12(4), 200–202.
Nunan, D., Sandercock, G. R., & Brodie, D. A. (2010). A quantitative systematic review of normal values for short-term heart rate variability in healthy adults. Pacing and clinical electrophysiology, 33(11), 1407–1417.
Olsen, M. F., Bjerre, E., Hansen, M. D., Hilden, J., Landler, N. E., Tendal, B., & Hróbjartsson, A. (2017). Pain relief that matters to patients: systematic review of empirical studies assessing the minimum clinically important difference in acute pain. BMC medicine, 15, 1-18.
Parkitny, L., & McAuley, J. (2010). The Depression Anxiety Stress Scale (DASS). Journal of Physiotherapy, 56(3), 204. https://doi.org/10.1016/S1836-9553(10)70030-8
Parkes, J., Hill, N. A. N., Platt, M. J., & Donnelly, C. (2010). Oromotor dysfunction and communication impairments in children with cerebral palsy: a register study. Developmental Medicine & Child Neurology, 52(12), 1113-1119.
Patrick, G. (1999). The effects of vibroacoustic music on symptom reduction. IEEE engineering in medicine and biology magazine, 18(2), 97-100.
Patwardhan, A. R., Vallurupalli, S., Evans, J. M., Bruce, E. N., & Knapp, C. F. (1995). Override of spontaneous respiratory pattern generator reduces cardiovascular parasympathetic influence. Journal of applied physiology, 79(3), 1048–1054.
Pearlin, L. I. (1989). The sociological study of stress. Journal of Health and Social Behavior, 30(3), 241–256.
Pelletier, C. L. (2004). The effect of music on decreasing arousal due to stress: A meta-analysis. Journal of Music Therapy, 41(3), 192–214. https://doi.org/10.1093/jmt/41.3.192
Penttilä, J., Helminen, A., Jartti, T., Kuusela, T., Huikuri, H. V., Tulppo, M. P., Coffeng, R., & Scheinin, H. (2001). Time domain, geometrical and frequency domain analysis of cardiac vagal outflow: effects of various respiratory patterns. Clinical physiology, 21(3), 365–376.
Porges, S. W. (2007). The polyvagal perspective. Biological psychology, 74(2), 116-143.
Tomaino, C. M. (2012). Using rhythmic auditory stimulation for rehabilitation. In Music, Science, and the Rhythmic Brain (pp. 111-121). Routledge.
Punkanen, M., & Ala-Ruona, E. (2012). Contemporary vibroacoustic therapy: Perspectives on clinical practice, research, and training. Music and Medicine, 4(3), 128-135.
Rajendra Acharya, U., Paul Joseph, K., Kannathal, N., Lim, C. M., & Suri, J. S. (2006). Heart rate variability: a review. Medical & biological engineering & computing, 44(12), 1031–1051.
Robe, A., Păsărelu, C. R., & Dobrean, A. (2021). Exploring autonomic regulation in children with ADHD with and without comorbid anxiety disorder through three systematic levels of cardiac vagal control analysis: Rest, reactivity, and recovery. Psychophysiology, 58(9), e13850.
Rogers, D. R. B., Ei, S., Rogers, K. R., & Cross, C. L. (2007). Evaluation of a multi-component approach to cognitive-behavioral therapy using guided visualizations, cranial electrotherapy stimulation, and vibroacoustic sound. Complementary Therapies in Clinical Practice, 13(2), 95–101. https://doi.org/10.1016/j.ctcp.2006.10.002
Rüütel, E. (2002). The psychophysiological effects of music and vibroacoustic stimulation. Nordic Journal of Music Therapy, 11(1), 16-26. https://doi.org/10.1080/08098130209478039
Saquetto, M., Carvalho, V., Silva, C., Conceição, C., & Gomes-Neto, M. (2015). The effects of whole body vibration on mobility and balance in children with cerebral palsy: a systematic review with meta-analysis. Journal of Musculoskeletal & Neuronal Interactions, 15(2), 137–144
Salleh, M. R. (2008). Life event, stress and illness. Malaysian Journal of Medical Sciences, 15(4), 9–18. PMID: 22589633
Sandler, H., Fendel, U., Buße, P., Rose, M., Bösel, R., & Klapp, B. F. (2017). Relaxation – Induced by Vibroacoustic Stimulation via a Body Monochord and via Relaxation Music – Is Associated with a Decrease in Tonic Electrodermal Activity and an Increase of the Salivary Cortisol Level in Patients with Psychosomatic Disorders. PLOS ONE, 12(1), e0170411. https://doi.org/10.1371/journal.pone.0170411
Sapolsky, R. M. (2004). Why zebras don’t get ulcers: The acclaimed guide to stress, stress-related diseases, and coping. Holt Paperbacks.
Selye, H. (1956). The Stress of Life. New York: McGraw-HillBook Co. Inc USA.
Selye, H. (1974). Stress without distress. In Psychopathology of human adaptation (pp. 137-146). Boston, MA: Springer US.
Shaffer, F., & Ginsberg, J. P. (2017). An overview of heart rate variability metrics and norms. Frontiers in Public Health, 5, 258. https://doi.org/10.3389/fpubh.2017.00258
Skille, O. (1989). VibroAcoustic Therapy. Music Therapy, 8(1), 61–77.
Dostupné online: https://academic.oup.com/musictherapy/article-pdf/8/1/61/8739474/8-1-61.pdf
Skille, O. (1991). Manual of Vibroacoustic Therapy. Levanger, Norway: ISVA Publications.
Skille, O. (1992). Vibroacoustic research 1980-1991. In R. Spintge, R. Dron (Eds.). Music and Medicine. St Louis, MO: MMB Music, Inc. Tiidus, P.M., Markoulakis, R., Murray, D., Bryden, P.J.
Skille, O. (1995). The Effect of Music, Vocalisation and Vibration on Brain and Muscle Tissue: Studies in Vibroacoustic Therapy. Teoksessa: Wigram, T., Saperston, B. & West, R.(Edit.) The Art and Science of Music Therapy: A Handbook.
Skille, O., Wigram, T., & Weekes, L. (1989). Vibroacoustic therapy: The therapeutic effect of low frequency sound on specific physical disorders and disabilities. Journal of British Music Therapy, 3(2), 6-10.
Smolík, P. (2002). Duševní a behaviorální poruchy: průvodce klasifikací, nástin nozologie, diagnostika. Maxdorf.
Thayer, J. F., Åhs, F., Fredrikson, M., Sollers, J. J., & Wager, T. D. (2012). A meta-analysis of heart rate variability and neuroimaging studies: implications for heart rate variability as a marker of stress and health. Neuroscience & Biobehavioral Reviews, 36(2), 747–756. https://doi.org/10.1016/j.neubiorev.2011.11.009
Thoits, P. A. (2010). Stress and health: Major findings and policy implications. Journal of Health and Social Behavior, 51(1_suppl), S41–S53.
Tomaino, C. M. (2012). Using rhythmic auditory stimulation for rehabilitation. In Music, Science, and the Rhythmic Brain (pp. 111-121).
Valenta, M., Müller, O., & Vítková, M. (2013). Metodika práce se žákem s mentálním postižením. Univerzita Palackého v Olomouci.
Veternik, M . , Misek, J., Jakus, J., Tonhajzerova, I., Jakusova, V., Hudečkova, H. (2018). The impact of sound exposure on heart rate variability in adolescent students. Physiological Research, 67, 695 - 702 DOI:10.33549/physiolres.933882
Vilímek, Z., a Chráska, M. (2019). Vliv vibroakustické stimulace na subjektivní vnímání. In Tělo a mysl. Sborník odborných příspěvků (s. 340–349). Olomouc: Univerzita Palackého v Olomouci.
Vilímek, Z., Kantor, J., a Chráska, M. (2019). Vliv vibroakustické stimulace na autonomní nervový systém. In Tělo a mysl. Sborník odborných příspěvků (s. 332–339). Olomouc: Univerzita Palackého v Olomouci.
Vilímek, Z., Kantor, J., Krejčí, J., Janečka, Z., Jedličková, Z., Nekardová, A., Botek, M., Bucharová, M., a Campbell, E. A. (2022). The effect of low frequency sound on heart rate variability and subjective perception: A randomized crossover study. Healthcare, 10, 1024. https://doi.org/10.3390/healthcare10061024
Vilímek, Z., Kořínková, J., a Kantor, J. (2021). The impact of vibroacoustic therapy on subjective perception of university students – Mixed design pilot study. Universal Journal of Educational Research, 9(7), 1409–1420. https://doi.org/10.13189/ujer.2021.090707
Vilímek, Z., Uhrinová, Z., Bucharová, M., Kantor, J., a Krejčí, J. (2023). Wirkung der vibroakustischen Therapie auf Spastik und Herzfrequenzvariabilität bei zwei jungen Erwachsenen mit Zerebralparese. časopis REHABILITÁCIA, 60(3), 1-15. https://doi.org/10.61983/lcrh.v60i3.11
Vítková, M. (2008). Speciální pedagogika. In S. Fischer & J. Škoda (Eds.), Speciální pedagogika (s. 5–10). Triton. https://knihovna.zcu.cz
Walters, C.L. (1996). The psychological and physiological effects of vibrotactile stimulation, via a Somatron, on patients awaiting scheduled gynecological surgery. Journal of Music Therapy, 33(4):261-287.
Warth, M., Kessler, J., Kotz, S., Hillecke, T. K., & Bardenheuer, H. J. (2015). Effects of vibroacoustic stimulation in music therapy for palliative care patients: A feasibility study. BMC Complementary and Alternative Medicine, 15, 436. https://doi.org/10.1186/s12906-015-0933-8
Wewers, M. E., & Lowe, N. K. (1990). A critical review of visual analogue scales in the measurement of clinical phenomena. Research in Nursing & Health, 13(4), 227–236. https://doi.org/10.1002/nur.4770130405
Wigram, T. (1995). The psychological and physiological effects of low frequency sound and music. Music Therapy Perspectives, 13(1), 16-23.
Wigram, A. L. (1996). The effects of vibroacoustic therapy on clinical and non-clinical populations (Doctoral dissertation, University of London).
Wigram, T. (1997). The Effect of Amplitude Modulation of the Pulsed Sinusoidal Low Frequency Tone as a Stimulus in Vibroacoustic Therapy. In T. Wigram, & C. Dileo. Music Vibration and Health (pp. 133-142). Jeffrey Books.
Wigram, T. (1997). The effect of vibroacoustic therapy compared with music and movement based physiotherapy on multiply handicapped patients with high muscle tone and spasticity. Music Vibration and Health. Cherry Hill, NJ: Jeffrey Books, 6985.
Wigram, T. (1997). The effect of VA therapy on multiply handicapped adults with high muscle tone and spasticity. In Music, Vibration and Health (p. 11).
Wigram, T., & Dileo, C. (1997). Music, vibration, and health. Cherry Hill, NJ: Jeffrey Books.
Wilder, J. (1967). Stimulus and response: The law of initial value. International Journal of Psychosomatics, 14(1), 11–20.
Young, F. L., & Leicht, A. S. (2011). Short-term stability of resting heart rate variability: influence of position and gender. Applied physiology, nutrition, and metabolism = Physiologie appliquee, nutrition et metabolisme, 36(2), 210–218.
Zafeiriou, D. I., & Batzios, S. P. (2013). Brain and spinal MR imaging findings in mucopolysaccharidoses: a review. AJNR. American journal of neuroradiology, 34(1), 5–13.
Zeidner, M. (2005). Test anxiety: The state of the art. Springer.

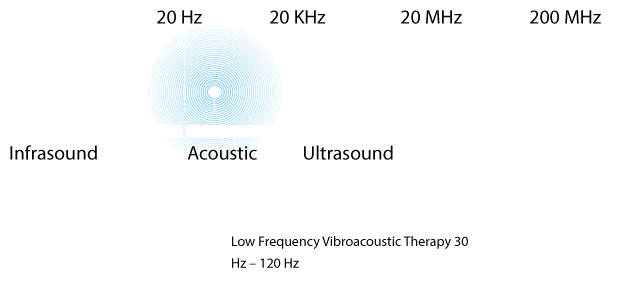



 Basic vibroacoustic therapy variables
Basic vibroacoustic therapy variables






 Kontaktní formulář
Kontaktní formulář
